Heart Disease in Indian Americans
Why Indians should be Concerned?
Because we are in the midst of a Cardiometabolic Epidemic!
High incidence of CardioMetabolic Syndrome with larger waist line(visceral fat), with or without Diabetes and with underlying excess of Insulin (Insulin Resistance), small dense LDL, remnant particles, proinflammatory, procoagulant factors contributes to the very high incidence of heart disease and all cause mortality in Indians.
The NIH program 'Healthy People 2010' designated the Asian Indian Immigrant Population in the United States as a "high risk group for heart disease".
The World Health Report of 2002 projects Cardio Vascular Disease (CVD=heart disease and stroke) to be the largest cause of death and disability in India by 2020.
The World Health Organization estimates that about 60% of the World's heart disease patients will be Indian by year 2010.
CVD is the largest cause of death in women. Compared to Whites, Blacks and Latinos Indian women suffered the highest all cause mortality and highest cardiovascular mortality in the U.S.
The Diabetes in Indian Americans study showed much higher age-adjusted prevalence of Metabolic Syndrome of 26.9% by the original ATP III criteria, 32.7% by the modified ATP III criteria and 38.2% by the IDF criteria.
Diabetes in Indian Americans
Premature and accelerated atherosclerosis, severe three vessel CAD,
diffuse coronary involvement, a higher relative rate of myocardial
infarction, severe left ventricular dysfunction, all seem to be much
more common in Asian Indians although the conventional risk factors such
as hypertension, smoking and consumption of red meets are less
prevalent in the same population.
However in recent years there has been an alarming increase in the number of people who smoke and drink in India. Consumption of salt,transfats, fast foods, red meats and animal fats and sedentary life style and childhood obesity are all on the rise in India!
Consumption of fresh vegetables and fruits is meager in many regions in India.
Heart unhealthy cooking and eating habits and lack of exercise and lack
of outdoor leisure time activities are highly prevalent and unmask
heart disease in Indians.
Treating dyslipidemias, diabetes and hypertension to goals is not a priority yet!
In the presence of large waist line,low HDL-C, high triglycerides, high blood pressure and insulin resistance, the threshold for the detrimental effects of LDL-C is lowered leading to an explosion of heart disease in India.
The population of India is over a Billion. Twenty million are living abroad. Two million Indians are living in USA (of these approximately 50,000 are physicians). Incidence of CAD in urban India is as high as it is in the Western World. Heart attack in one or more members of many Indian families has become an accepted adverse event! Even after the diagnosis of CAD has been made optimum treatment is not being delivered. This does not have to be the case anymore. There is no reason to wait any longer to start a global, well-coordinated fight against CAD in Asian Indians.CAD in Indians is reaching epidemic proportions!
What are the Reasons to Start the RICADIA Project?
- Asian Indians have the highest risk of CAD and it also starts at an early age.
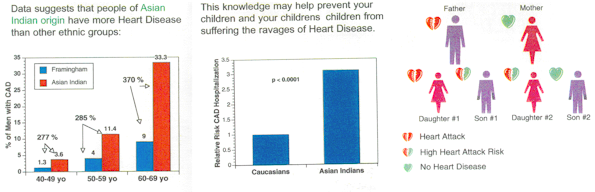
- Hospitalization rate of CAD among Asian Indians in US is four times higher than Caucasians, Japanese and Filipinos and five times higher than Chinese.
- Asian Indian women, vegetarians and nonsmokers are also at high risk of CAD and its complications.
- Earliest identification & aggressive treatment of CAD is very important to prevent morbidity & mortality that results from this number one killer disease.
- The general guidelines do not address the risk factors and life styles unique to Asian Indians. Therefore many Indian patients will go unrecognized and untreated. RICADIA Project is created to address these problems specific to Asian Indians and provide them with specific guidelines and therapeutic life habits customized to each individual to achieve timely and maximum prevention of heart disease.
What are the Risk Factors for CAD in General?
- High LDL or bad cholesterol
- Smoking
- Metabolic syndrome
- High blood pressure
- Diabetes
- Family history of CAD
- Menopause (Change of life) in women.
What Risk Factors for CAD are Common in Asian Indians?
- Low HDL cholesterol (good cholesterol)
- borderline high LDL cholesterol (bad cholesterol)
- High VLDL, Triglycerides (ugly cholesterol)
- Metabolic (Central Obesity-Insulin resistance) syndrome
- Diabetes and pre-diabetes
- Sedentary Life Style
- Unhealthy Culinary Practices
Why Life Long Vegetarians Have to Worry About Heart Disease.
Their risk is identical to that of a non-vegetarian.
What is Lp(a)?
When present in excess quantities in blood it favors premature fatty deposition (Atherosclerosis), and blood clotting in the blood vessels (thrombosis), it is also responsible for the high failure rate of balloon angioplasty and coronary artery bypass surgery. However DIA(Diabetes in Indian Americans)- the first randomized, multicenter, national study in the U.S showed no statistical significance as a risk factor for Lp(a)in Indians. But the Diabetes in Indian Americans study showed much higher age-adjusted prevalence of Metabolic Syndrome of 26.9% by the original ATP III criteria, 32.7% by the modified ATP III criteria and 38.2% by the IDF criteria.
What is Metabolic (central obesity-insulin resistance) Syndrome?
Learn about Metabolic Syndrome
Indian Americans and CardioMetabolic Syndrome Brochure
Larger your waist line shorter is your life span!
Indian Food Nutrition Information
What is Primary Prevention and What is Secondary Prevention?
Primary prevention is to identify individuals at risk for CAD at an early stage before symptoms and signs of CAD appear, identify their risk factirs for CAD and provide them with specific diet, life style, and pharmacological advice as indicated by their test results. Secondary prevention is for patients who already have symptoms and signs of CAD. These are angina (chest pain), Myocardial Infarction (heart attack), heart failure, heart rhythm disturbances and cardiac disability. Besides diet and life style advice these patients are provided with pharmacological treatment with the following medications, interventions and devices as indicated.
- Statins: to reduce cholesterol and plaque burden.
- Beta Blockers: to reduce angina, prevent recurrent heart attack and sudden cardiac death.
- Nitroglycerine compounds: to relieve angina & heart failure.
- Calcium channel blockers: to relieve angina.
- ACE Inhibitors and Angiotensin Receptor Blockers: to improve signs and symptoms of heart failure, help favorable remodeling of heart muscle and pumping function after a heart attack and to prolong life.
- Aspirin and Glycoprotein 2b 3a inhibitors: to prevent thrombosis(blood clotting) in the coronary arteries.
- Balloon Angioplasty/Stent and Coronary Artery Bypass Graft surgery: To reestablish blood flow through previous blockages.
- Implantable devices: Cardiac Defibrillators to prevent life threatening arrhythmias and Biventricular Pacing to improve heart pumping.
- Heart transplant: for people with severe cardiac dysfunction
- Cardiac rehabilitation: For patients with cardiac disability.
Obviously primary prevention is the best prevention!
Summary of RICADIA Project
- Asian Indians have the highest risk of heart disease among all ethnicities and women, vegetarians and non smokers are no exception.
- Sedentary life styles and unhealthy cooking habits contribute a great deal of heart disease in Asian Indians. High incidence of metabolic syndrome, pre-diabetes and diabetes in Asian Indians.
- Aim of the RICADIA project is to help identify the individual and family at risk for heart disease and provide specific diet, lifestyle and pharmacologic advice customized to each subject to prevent heart disease at the earliest stage possible.
- Remember, it is never too early when it comes to prevent heart disease because 'fatty streaks' appear as early as in the second trimester of intrauterine life in fetuses of mothers who have high cholesterol.
Who Should be Tested / Contact Information for RICADIA Project?
People from India, Pakistan, Sri Lanka and Bangladesh. Please call (619) 229-1995 or email pkotha@heartsmart.info.
Your proactive role is important to prevent premature disability and deaths associated with Coronary Artery Disease. Please share this information with your family and friends.
Contributions made to RICADIA are tax deductible and are utilized for the betterment of society. Please take charge of your health and be part of the solution. Checks should be made payable to RICADIA project and mailed to:
RICADIA Project
5555 Reservoir Drive, Suite 309
San Diego, CA 92120
Please call (619) 229 1995 or email any questions to director@ricadia.org or pkotha@heartsmart.info

|
HeartSmart targets at risk Asians.docx 2.docx Size : 13.963 Kb Type : docx |

|
Ind Ame C Met S 2014.pdf Size : 1159.558 Kb Type : pdf |